
How Breathing & Physical Health Interact
Highlights:
- Breathing affects physical health through 3 fundamental mechanisms. The excitation of the central nervous system, the mechanical movement of the diaphragm, and the regulation of our blood’s chemistry.
- These three pathways can become the source or a significant contributor to several conditions, from lower back pain to allergic reactions, inflammation, and cardiovascular disease.
- Breathing correctly is thus a fundamental mechanism for maintaining healthy blood chemistry, nervous system balance, and abdominal function.
Humans have widely leveraged the connection between breathing and physical health throughout millennia as a healing tool for the disorders of our body and the soul. Our previous article, “Breathing & Psychological Stress: A two-way street,” described the physiological processes that connect the brain and breathing, enabling us to control stress levels and emotions by deliberately changing our breathing. However, a set of similar functions can also heavily influence other core physiological processes that can impact our physical health.
The scientific community’s renewed interest in the mechanics and biology of breathing has shed light on the fundamental mechanisms connecting respiration and the mind and those connecting respiration and physical health. By analyzing them, we can begin to understand how chronic inflammation and over-excitation of our immune system lead to auto-immune disorders, lower back pain, digestion disorders, and more.
As a first step, let’s understand the fundamental biomarkers that characterize how healthy our breathing process is. These include:
- End-tidal CO2: The amount of carbon dioxide we exhale.
- Tidal volume: The volume of air we exhale.
- Breathing frequency: The number of breaths we take per minute.
These biomarkers reflect our breathing health because they constitute the basic mechanisms by which breathing affects nearly everybody process, including digestion, immune response, mitochondrial function, cardiovascular health, and hormonal balance. To understand how all these systems are affected by our breathing, let’s examine, step by step, the sequence of events occurring when the three fundamental breathing variables are perturbed from their average values.
How Breathing Affects The Nervous System
Breathing and the autonomic nervous system (ANS) are inextricably linked through various mechanisms. ANS is divided into two parts: the Sympathetic Nervous System (SNS) and the Parasympathetic Nervous System (PNS). SNS causes us to go into “fight-or-flight” mode by engaging all the mechanisms required for movement, preservation, and fast reaction. Conversely, PNS causes feelings of relaxation and enables us to recover, digest, and heal. The link between ANS and breathing is made possible through how the neurons connect to the different lung parts. Specifically, SNS is connected to the upper part, whereas PNS is connected to the lower lungs. Due to the anatomy of the connection between lungs, SNS, and PNS, we engage SNS and partially deactivate PNS when we breathe faster and shallower. On the contrary, when we deliberately breathe deeper and slower, we can activate PNS thanks to its connection to the lower part of our lungs and thus enable feelings of relaxation.
Breathing continuously faster and shallower, a condition called Chronic Hyperventilation Syndrome (CHS), causes a chronic hyper-activation of SNS, setting our body in a perpetual state of increased stress. Engagement of SNS signals to our body the presence of danger and thus triggers a chain of reactions to prime us for facing it. Although these processes have been developed over thousands of years of evolution and can be lifesaving given their effect of setting us ready to respond to threats, their constant activation causes a cascade of negative repercussions. Here are the main mechanisms and physiological systems affected:
- Digestive System: The engagement of SNS causes blood to leave the stomach and core and is channelled to the brain and muscles to render our body ready to think and react fast. Stomach ischemia (lack or absence of blood) causes digestion to slow or halt, leading to chronic digestion and gastrointestinal issues.
- Cardiovascular System: Engagement of the SNS increases blood pressure to render our muscles better able to reach fast and respond to threats. However, a chronic increase in blood pressure leads to hypertension, eventually leading to life-threatening cardiovascular conditions such as coronary artery disease. Moreover, irregular breathing patterns can lead to diaphragmatic atrophy, in which the diaphragm moves less, adding additional strain to the heart.
- Immune System: Engagement of the SNS also engages our immune system through the Hypothalamic-Pituitary-Adrenal (HPA) axis. The HPA axis is the conglomeration of three critical physiological systems, namely the Hypothalamus, the Pituitary, and the Adrenal gland, that cooperate to convert brain signals and stimuli into physiological responses necessary to elicit the appropriate bodily reaction. When stress stimulus occurs
- Endocrine regulation: Engagement of the SNS also impacts our hormones critical to the endocrine balance through the Hypothalamic-Pituitary-Adrenal (HPA) axis. The HPA axis is the conglomeration of three crucial physiological systems, namely the Hypothalamus, the Pituitary, and the Adrenal gland, that cooperate to convert brain signals and stimuli into physiological responses necessary to elicit the appropriate bodily reaction. When a stress stimulus is perceived through the hypothalamus, it sends an alert to the pituitary gland through the corticotropin-releasing hormone (CRH). In addition to stimulating the sympathetic nervous system, CRH will stimulate the pituitary gland and cause it to release adrenocorticotropic hormone (ACTH). ACTH travels through the body and targets the adrenal gland causing them to release cortisol. When stress is constantly elevated, cortisol levels will remain high and induce a cascade of adverse effects, including:
- Suppression of reproductive function
- Increase in insulin resistance, a precursor to diabetes
- Suppression of growth and thyroid hormone release impedes development, physical recovery, and thyroid function.
- Immune system hyperactivation: Our central nervous system is also interconnected with our immune system through a molecule called Cytokines. Cytokines are a general category of small proteins that play an essential role in cell signalling. They control the growth and activity of immune blood cells, enabling them to trigger inflammation and respond to pathogens. Overactivation of the sympathetic nervous system can, therefore, result in constant activation of the immune system, leading to
chronic inflammation and auto-immune disorders.
How Mechanics Of Breathing Affect Our Body
In addition to the nervous-based interaction between breathing and several key sectors of our physiology, breathing also affects our health through the mechanics of respiration.
- Cardiovascular Strain: One of the most critical systems in our breathing apparatus is the diaphragm, a dome-shaped muscle between the lungs and the abdominal area. The diaphragm moves down and up, and we inhale and exhale. Our abdomen contains 25-30% of our body’s total blood volume, making it one of the most blood-dense areas of our body. Rapid and shallow breathing reduces the engagement of the diaphragm and can, over time, lead to diaphragmatic atrophy, the state where the diaphragm weakens and moves less during respiration. The movement of the diaphragm aids in abdominal blood circulation, representing a significant part of the overall blood circulation in our body. This is why the diaphragm is also referred to as the second heart. As a result, diaphragmatic atrophy leads to a minor contribution of the diaphragm on blood circulation and thus increases the load our heart has to support whole-body circulation.
- Posture and skeletal muscular disorders: The diaphragm is a critical component of our breathing apparatus. Strong diaphragmatic engagement increases abdominal pressure, engages the abdominal muscles, and thus provides support to our core and lower back. On the contrary, weak diaphragmatic movement caused by shallow breathing weakens our core stability and is a key factor for developing lower back pain and other skeletal muscle disorders.
- Brain oxygenation: Breathing and hyperventilation is the primary regulator of the blood's balance between oxygen and carbon dioxide. As breathing becomes faster, the air exhaled increases along with the amount of carbon dioxide (CO2) expelled through the body. As more CO2 leaves the body, CO2 circulating in the blood declines, causing a cascade of adverse effects as it is responsible for two critical biological functions. First, CO2 enables oxygen molecules to detach from hemoglobin (the substance in our blood responsible for transporting oxygen from our lungs across the body) and enter the cells that need them to produce energy. Second, CO2 regulates how narrow or wide our arteries are and the amount of blood delivered across the body. As a result, reducing, making it harder for oxygen to enter cells and narrowing the arteries, diminishing blood delivery to the brain and across the body.
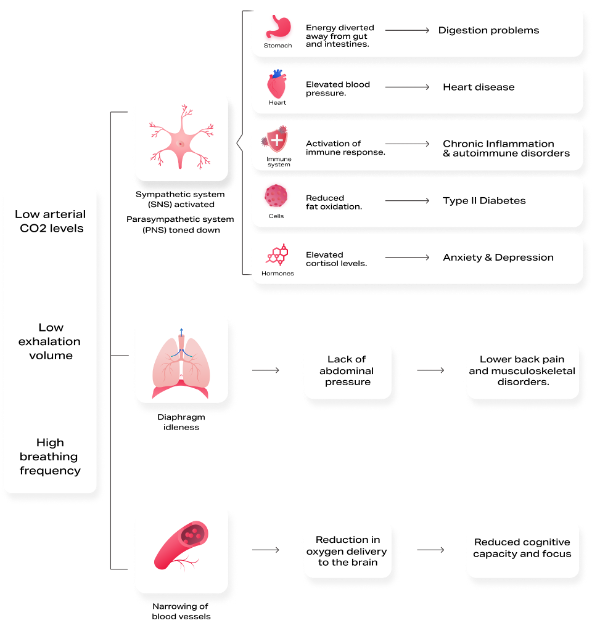
The following graph provides a summary of how these mechanisms interact with each other:
Conclusion
Breathing is a crucial regulator of several critical functions, including blood chemistry, nervous system balance, and abdominal pressure. Learning how to breathe in accordance with your metabolic needs can become a healing factor for many psychosomatic disorders and prevent the onset of chronic conditions. As a result, breathing is the most influential physiological function that’s in your control.
An Ounce of Prevention - Hyperion Health Blog



